2025 Printable Template
This website is not affiliated with any government agency or tax authority.
Form last updated: 03/2024. Please verify this is the current version before use.
Easily complete & submit your DD 2870 form
Follow these simple steps to fill, sign, and send your DD 2870 form online.
Fill out your form
Our user-friendly editor helps you quickly enter personal & business details in the DD 2870 template.
Sign the form
Add your electronic signature to the fillable DD 2870 form to certify it came directly from you.
Send it to the requester
Download and instantly print or share your signed DD 2870 with the requester.
How to fill out a DD 2870 online?
Follow these steps to complete your DD 2870 form online.
Step 01
Access the form online and open it in the PDF editor.
Step 02
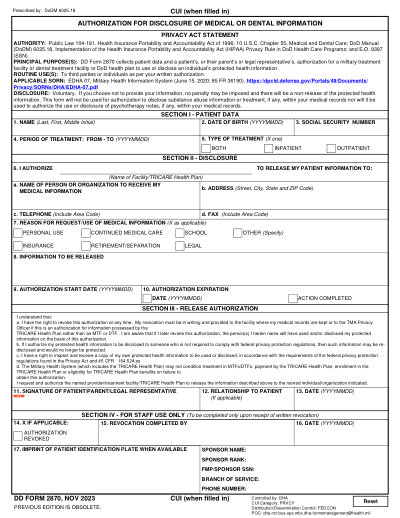
Fill in the patient's name and date of birth in the designated fields.
Step 03
Enter the sponsor's Social Security Number.
Step 04
Specify the treatment dates or select 'ALL TIME PERIODS'.
Step 05
Indicate whether you need outpatient or inpatient records.
Step 06
Provide the reason for the request and the recipient's details.
What is a DD 2870 used for?
Who needs to fill out a DD 2870 form
What information do I need to provide in Section I?
Who can receive my medical information?
Can I revoke my authorization?
Ready to Fill Your Form DD 2870?
Start filling out your form online in minutes. Fast, secure, and completely free.
Our users speak for themselves
Exceptional quality verified by real professionals.
"The editing was very easy and easy to download the document."
Fouzia Barwari
Jun 2, 2026
"Quick easy and straightforward thank you"
MRS DAWN ANDREWS
May 23, 2026
"Simple efficient process. It all worked."
Sundeep Salins
Jun 3, 2026
"Editing was easy. I changed some text in the file without affecting the original font or page layout"
Bhagya
May 14, 2026